
This week in Closer Looks we’ll dive into NJ S1830, relating to requiring certain schools maintain a supply of opioid antidotes. This comes as a result to our growing national epidemic surrounding opioids. States have spent the last few years grappling with this issue and proposing legislation aimed at curbing use, studying the effects of it on our people and educating the professionals with access to these substances.
How did We Get Here?
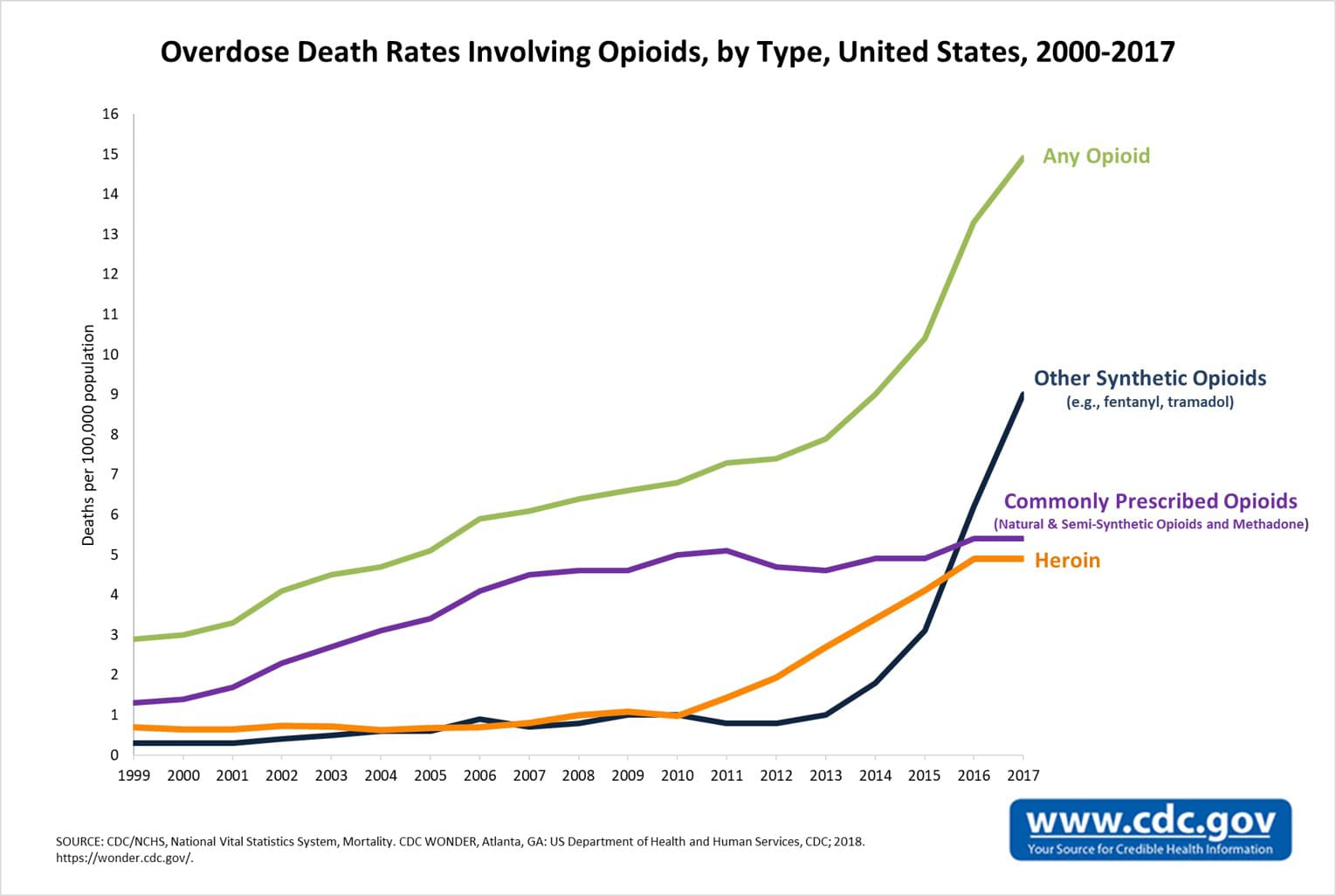
In the late 1990s, pharmaceutical companies reassured the medical community that patients would not become addicted to opioid pain relievers and healthcare providers began to prescribe them at increasingly higher rates. When looking at “opioids”, think of drugs like prescription pain relievers, heroin and synthetic opioids like fentanyl. We now live in a country where every day more than 115 people die after an opioid overdose. In 2017 HHS declared a public health emergency and announced a 5-Point Strategy To Combat the Opioid Crisis.
{kind=link}

The Centers for Disease Control and Prevention estimates the total “economic burden” of prescription opioid misuse in the US is $78.5 billion a year. These costs are attributed to healthcare, lost productivity, addiction treatment and criminal justice involvement.
What is Being Done?
Take a look at what different states and countries around the world are doing relating to drug addiction and how Jeff Session’s war on marijuana relates to this issue.
Two previously trending bills this year also had to do with limiting the prescription of opioids. A Florida bill aimed to require each person registered with the US Drug Enforcement Administration and authorized to prescribe controlled substances, to complete a board-approved 2-hour continuing education course on prescribing controlled substances. The courses must specialize in current standards for prescribing controlled substances, particularly opiates, and alternatives to these standards. A Louisiana bill also provided limitations on prescribing opioids. It states a medical practitioner cannot prescribe more than a seven-day supply to an adult patient when issuing a first-time opioid prescription for outpatient use. When it comes to minors, they cannot issue a prescription for an opioid for more than a seven-day supply at any time. They also will need to discuss with a parent, tutor or guardian of the minor risks associated with opioid use and the reasons why the prescription is necessary.
Another Louisiana bill creates the Advisory Council on Heroin and Opioid Prevention and Education. It allows the council to engage and solicit input, recommendations, and guidance pertaining to heroin and opioid prevention and education from interested parties and stakeholders. They will need to establish an “Interagency Heroin and Opioid Coordination Plan” and a “central online location to disseminate information and resources”.
Naloxone, the most common opioid antidote, is a medication designed to rapidly reverse an opioid overdose. It is an opioid antagonist—meaning it binds to opioid receptors and can reverse and block the effects of other opioids. There are three FDA approved methods of administering Naloxone, injectable (which requires training), auto-injectable (like EVZIO® – a prefilled auto-injection device allowing quick injection into the outer thigh) or prepackaged nasal spray (like NARCAN® Nasal Spray – a prefilled, needle-free device that requires no assembly and is sprayed into one nostril while patients lay on their back).
How does this Affect the Children?
Of the estimated 2.1 million Americans currently addicted to opioids, the young-adult population has been hit hardest. Nearly 400,000 adults ages 18 to 25 suffer from addiction to prescription painkillers (most common) or heroin. Researchers found the number of children admitted to hospitals for opioid overdoses nearly doubled. The 797 patients between 2004 and 2007 moved up to 1,504 patients between 2012 and 2015 .
NJ S1830 requires certain schools to maintain a supply of opioid antidotes and permits emergency administration of opioid antidote by a school nurse or trained employee.
The policy will:
- Require a school that includes any of the grades nine through 12, and permit any other school to obtain a standing order for opioid antidotes and to maintain a supply of opioid antidotes in a secure and easily accessible location
- Permit the school nurse or trained employees to administer an opioid antidote to any person whom the nurse or trained employee in good faith believes is experiencing an opioid overdose
The guidelines will require each school nurse, and each employee designated by the board of education, board of trustees of a charter school or chief school administrator of a nonpublic school, receive training on standardized protocols for the administration of an opioid antidote to a person who experiences an opioid overdose. The bill also provides immunity from liability for school nurses and other employees or agents. The training will include the overdose prevention information described in the “Overdose Prevention Act.”
Here is a map of all the current legislation having to do with opioids and schools.